
1. BACKGROUND
The rubella virus is the etiologic agent of a mild rash with low-grade fever, lymphadenopathy, and morbidity rash, which was first described in the late 18th century and was called by Bergen, a German physician, Rutheln. The first researchers to diagnose the disease from other exanthemas were German physicians; hence, the name is “German measles” in English [1]. In 1841, a British physician coined the term rubella, a Latin name meaning little red. In 1941, Gregg Norman, an Australian ophthalmologist, linked congenital cataracts to maternal rubella. In later years, the British, Australian, Swedish, and American epidemiologists and teratologists confirmed the role of rubella in cataracts and also found a link between concomitant heart disease and deafness in newborns. Therefore, the three characteristics of congenital rubella were determined [2]. Vaccination has had a major impact on the epidemiology of rubella since the late 1970s [3].
Rubella is a benign disease among children and adults. Acquired rubella infection affects two areas in which the immune system can be affected. The first area in the nasopharynx is where the virus first replicates and from there spreads to the local lymph nodes. The initial rubella infection is usually asymptomatic but can cause serious problems in pregnant women [4]. Uterine infections are one of the most important causes of perinatal complications and fetal death, especially in developing countries [5,6]. The immune system is temporarily suppressed during pregnancy, which makes pregnant women more vulnerable to infectious agents [7].
Among these pathogens, the prevalence of Toxoplasma gondii, rubella, and cytomegalovirus is very high and may cause congenital malformations, recurrent miscarriages, and preterm births [8,9].
Rubella can be a mild infectious disease that develops after childhood vaccinations [10]. Rubella infection during pregnancy is followed by severe manifestations such as recurrent miscarriages, intrauterine death, skeletal abnormalities, and lake of fetal development [11,12].
One of the common methods of diagnosis and screening of women in terms of these infectious agents is serological tests and measurement of specific antibodies to rubella virus[5,13].
Due to the effects of rubella infection on fetal health and pregnancy, screening of women for immunity to rubella virus and vaccination if necessary is very important [14]. The aim of this study was to evaluate the level of rubella antibodies in women referred to the gynecology clinic. The study population included women who were referred to the laboratory for prepregnancy tests.
2. MATERIALS AND METHODS
The study group included all women who were referred to the Al-Mahdi Women’s Clinic in the south of Tehran in the interval of 9 months in 2020. They were 140 women who were referred to the laboratory for prepregnancy tests. One of the prepregnancy tests was to determine the amount of serum rubella antibodies of both types immunoglobulin G (IgG) and Immunoglobulin M (IgM). The mentioned antibodies were tested by quantitative immunoassay using Immulite 2000 autoanalyzer (Siemens, Munich, Germany), according to the kit manufacturer’s instructions. All positive and suspicious results of antibodies were tested again.
Results for IgG and IgM rubella antibodies were interpreted according to manufacturer’s instructions as follow: for IgG (nonreactive: < 6.5, inter: 6.5–8, and positive: > 8) and for IgM (nonreactive: < 0.9, inter: 0.9–1.1, and positive: > 1.1). Statistical analysis was performed using Statistical Package for the Social Sciences software.
3. RESULTS
The mean age of women in this study was 29.09 years. 66.4% of women had a history of rubella vaccination in childhood, 18.6% had not been vaccinated, and 15% of the studied women did not know if they had been vaccinated. The mean age and distribution of age in studied women are shown in Table 1.
The frequency distribution of IgG antibody positive (> 8 ng/dl) and IgM antibody positive (> 1.1 ng/dl) in studied women was shown in Table 2.
The percentage of women who have been vaccinated is shown in Table 3. As shown in the result, 66.4% of the women studied had a history of rubella vaccination.
There was a significant association between rubella-vaccinated women and positive IgG antibody (p-value < 0.05), but there was no significant association between rubella-vaccinated women and positive IgM antibody (p-value < 0.05) in the studied group (Table 4).
 | Table 1: Distribution of age in women. [Click here to view] |
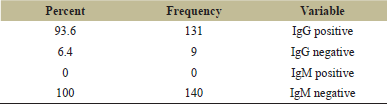 | Table 2: Frequency distribution of IgG antibody positive (> 8 ng/dl) and IgM antibody positive (>1.1 ng/dl) in studied group. [Click here to view] |
In our studied group of women, for 1 year of increasing age, the amount of antibody increases 0.02 ng/dl. Therefore, there was no significant relationship between increasing age and positive antibody cases (p-value < 0.05).
4. DISCUSSION
The rubella virus normally has a limited host domain (human only), but in the laboratory, it grows in a range of primary, semicontinuous, and persistent cells of pedigree origin. In human amniotic cells, they are suitable for continuous plaque formation in persistent cells, including rabbit kidney (RK-13) and hamster kidneys (BHK-21) [1]. During viremia (the presence of the virus in the blood and the onset of fever) in a pregnant woman, the virus often infects the placenta. Replication is thought to be a precursor to fetal infection, which leads to the entry of the virus into the fetal bloodstream and thereby infects fetal organs. Endothelial cell destruction leads to vasculitis and ischemia. In summary, the action of the rubella virus in organogenesis is mediated by a variety of factors, including intracellular pathology, proliferation, and apoptosis [2].
Serologic diagnosis depends on a fourfold increase in serum IgG titer between acute and recovery stages or the presence of IgM antibodies in acute stage samples [15]. Congenital rubella infection in infants is diagnosed with detection of virus, viral genome, IgM antibodies, and IgG antibodies with low avidity. The negative result of poly clonal chain reaction (PCR) performed on embryonic or amniotic fluid samples during pregnancy is good evidence against intrauterine rubella infection [16].
Prior to the implementation of immunization programs and rubella vaccination, it was endemic in the world on a regular and seasonal basis, occurring in temperate climates during the spring months. Prior to vaccination, rubella epidemics affected about 5% of the population, although only about 10% of these cases were reported to public health authorities. In many countries, vaccination with the triple vaccine, which includes measles, rubella, and mumps Vaccine (MMR) viruses, is given.
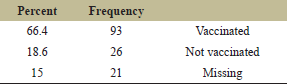 | Table 3: Frequency distribution of rubella vaccination in studied group. [Click here to view] |
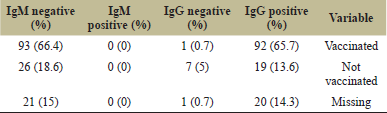 | Table 4: Statistical analysis between history of Rubella vaccination and IgG or IgM antibodies in studied group. [Click here to view] |
The triple formulation of the vaccine developed at the Razi Institute in Iran includes the infectious attenuated measles virus (ALK-TCID50 1000), mumps virus (HOSHINO-TCID50 5000), and rubella virus (TAKAHASHI TCID50 1000). Formulations in Europe and elsewhere with viral strains are different but available with the same infectious dose in the vaccine. Three vaccines against measles, rubella, and mumps have been prepared in Razi Institute since 1991. Prior to this date, imported vaccines were used. In short, the reaction was very mild after the injection and only a 1- or 2-day fever and a small rash, usually seen 2 weeks after the measles injection, are seen in these children. Rarely, transient unilateral swelling of the ear gland is seen in the third week after inoculation. According to the research conducted on the serum of vaccinated children, the serum of most of these children had antibodies against all three diseases 6 weeks after vaccination. This means that children are safe in this regard against all three diseases.
In this study, due to the importance of rubella in pregnant women, we decided to survey the level of immunity of some Iranian young women who want to become pregnant. The rubella vaccine or MMR vaccine is given in Iran in childhood in two times at 12 and 18 months of age and whether these people are immune in adulthood is not clear; therefore, the amount of serum antibodies should be measured in women who want to pregnant. In the early years of rubella vaccine production and distribution in Iran, because it was not free and paid for, children from some low-income families were not vaccinated.
In Iran, following the observation of cases of measles in adulthood in the second half of 2003, the largest measles-rubella vaccination program in the world was implemented, in which more than 33 million people aged 5–25 years were vaccinated in this program.
The main vaccination schedule is based on the fact that a booster dose should be given every 10 years. However, inoculation of the booster dose is not performed by all individuals. Therefore, according to the protocol of the Ministry of Health in Iran, all women who want to become pregnant perform a series of tests, including measuring the amount of antibodies against the rubella virus.
Therefore, according to the results of the present study, the rubella vaccination program in childhood as well as the general vaccination program for people aged 5–25 years, which was performed in Iran in 2003, was very effective and the majority of women were safe against rubella before pregnancy. Only a small percentage of the women studied did not have enough antibodies for various reasons. This limited number of unsafe women can also be immunized by injecting a booster dose of rubella vaccine [17].
5. ACKNOWLEDGMENTS
The author would like to thanks Miss Hourieh Khalili who helped us in this project.
6. ETHICS APPROVAL AND CONSENT TO PARTICIPATE
All women studied have signed a consent form. This study was approved by local conventional manner and by the ethical committee of Tehran University of Medical Sciences with number IR.TUMS.SPH.REC.1397.093
7. AUTHOR CONTRIBUTION
RM conceived and designed the study. K.K performed the research. All the authors approved the paper.
8. CONSENT FOR PUBLICATION
All the authors approved the paper.
9. AVAILABILITY OF DATA AND MATERIALS
All data and information are available.
10. CONFLICT OF INTEREST
The authors declare that they have no conflict of interest.
11. FUNDING
There has been no financial support for this work.
REFERENCES
1. Fields BN, Knipe DM, Howley PM. Fields virology. 5th edition, Wolters Kluwer Health/Lippincott Williams & Wilkins, Philadelphia, PA, 2007.
2. Plotkin S, Orenstein W, Offit P. Vaccines. 6th edition, Saunders, Philadelphia, PA, 2012.
3. Lochlainn LMN, de Gier B, van der Maas N, Strebel PM, Goodman T, van Binnendijk RS, et al. Immunogenicity, effectiveness, and safety of measles vaccination in infants younger than 9 months: a systematic review and meta-analysis. Lancet Infect Dis 2019;19(11):12345–45. CrossRef
4. Ocak S, Zeteroglu S, Ozer C, Dolapcioglu K, Gungoren A. Seroprevalence of Toxoplasma gondii, rubella and cytomegalovirus among pregnant women in southern Turkey. Scand J Infect Dis 2007;39(3):231–4. CrossRef
5. Sharma S, Duggal N, Agarwal S, Mahajan RK, Anuradha, Hans C. Seroprevalence of Toxoplasma, rubella and CMV infections in antenatal women in a tertiary care hospital in North India. J Commun Dis 2015;47:23–6.
6. Aynioglu A, Aynioglu O, Altunok ES. Seroprevalence of Toxoplasma gondii, rubella and cytomegalovirus among pregnant females in north-western Turkey. Acta Clin Belg 2015; 70:321–4. CrossRef
7. Mellor AL, Munn DH. Extinguishing maternal immune responses during pregnancy: implications for immunosuppression. Semin Immunol 2001;13(4):213–8. CrossRef
8. Calimeri S, Capua A, La Fauci V, Squeri R, Grillo OC, Giudice DL. Prevalence of serum anti-rubella virus antibodies among pregnant women in southern Italy. Int J Gynaecol Obstet 2012;116(3):211–3. CrossRef
9. Rahimkhani M, Khavari-Daneshvar H, Sharifian R. Asymptomatic bacteriuria and pyuria in pregnancy. Acta Med Iran 2008;46(5):409–12.
10. Hamdan HZ, Abdelbagi IE, Nasser NM, Adam I. Seroprevalence of cytomegalovirus and rubella among pregnant women in western Sudan. Virol J 2011;8(1):217. CrossRef
11. Uyar Y, Balci A, Akcali A, Cabar C. Prevalence of rubella and cytomegalovirus antibodies among pregnant women in northern Turkey. New Microbiol 2008;31(4):451–5.
12. Calimeri S, Capua A, La Fauci V, Squeri R, Grillo OC, Giudice DL. Prevalence of serum anti-rubella virus antibodies among pregnant women in southern Italy. Int J Gynaecol Obstet 2012;116(3):211–3. CrossRef
13. Karad D, Kharat A. Seroprevalence of torch infections in bad obstetrics history in HIV and Non-HIV women in Solapur District of Maharashtra India. J Hum Virol Retrovirol 2015;2:00067. CrossRef
14. Carazo S, Billard MN, Boutin A, De Serres G. Effect of age at vaccination on the measles vaccine effectiveness and immunogenicity: systematic review and meta-analysis. BMC Infect Dis 2020;20:251. CrossRef
15. Medici MC, Martinelli M, Albonetti V, Chezzi C, Dettori G. Evaluation of rubella virus immunoglobulin G (IgG) and IgM assays with the new vidia instrument. J Clin Microbiol 2008;46(5):1847–9. CrossRef
16. Rahimkhani M, Mordadi A, Gilanpour M. Detection of urinary Chlamydia trachomatis, mycoplasma genitalium and human papilloma virus in the first trimester of pregnancy by PCR method. Ann Clin Microbiol Antimicrob 2018;17(1):25. CrossRef
17. Abu-Elyazeed R, Jennings W, Severance R, Noss M, Caplanusi A, Povey M, et al. Immunogenicity and safety of a second dose of a measles-mumps-rubella vaccine administered to healthy participants 7 years of age or older: a phase III, randomized study. Hum Vaccin Immunother 2018;14(11):2624–31. CrossRef